SJS & TEN Spectrum Classifier
Select the percentage of Total Body Surface Area (TBSA) affected to see the classification and associated clinical risks.
Imagine waking up with a mild fever and a scratchy throat, thinking it is just a common cold. Within a few days, a red, painful rash spreads across your body, and your skin begins to peel away in sheets, similar to a severe burn. This is the terrifying reality of Stevens-Johnson Syndrome is a rare, life-threatening skin reaction typically triggered by a medication that causes the skin to blister and peel.
When this reaction becomes even more severe, it is known as Toxic Epidermal Necrolysis (TEN). While these conditions are rare, they are absolute medical emergencies. If you or a loved one are taking high-risk medications, knowing the difference between a simple drug rash and a systemic emergency can literally save a life. The goal is simple: recognize the signs early, stop the causative drug immediately, and get to a hospital.
Key Takeaways for Immediate Action
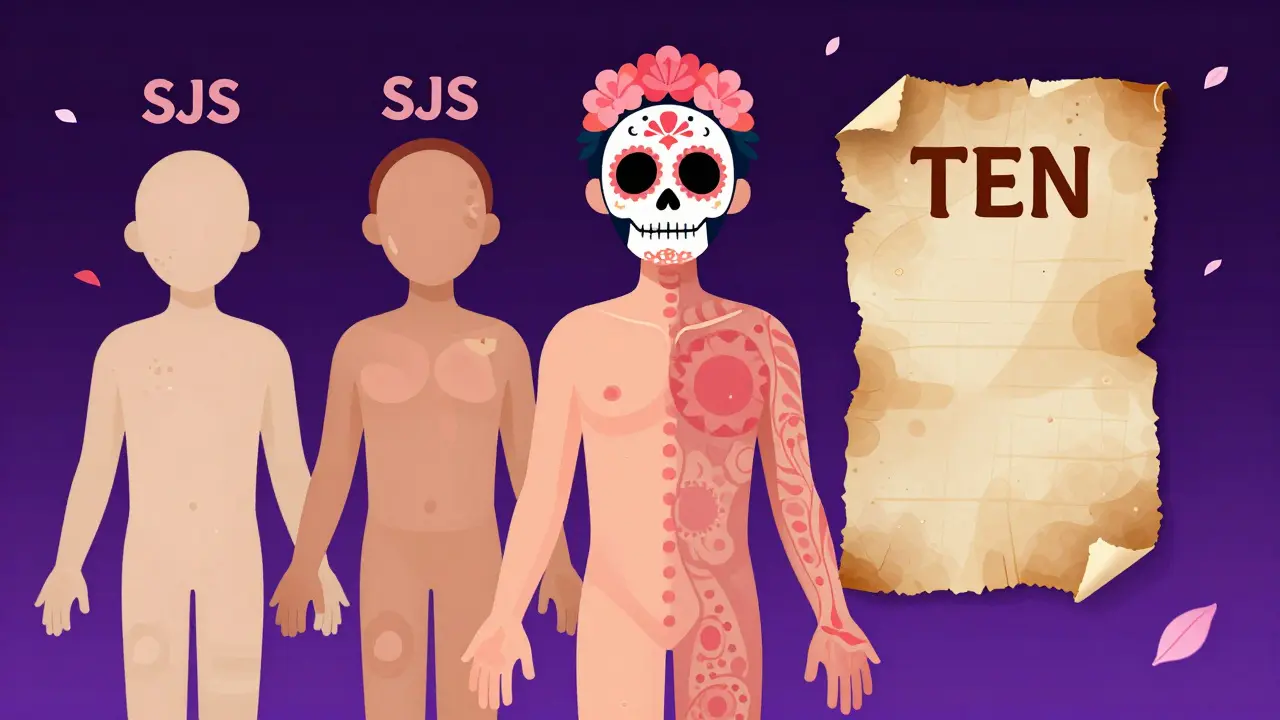
- SJS and TEN are on the same spectrum; the difference is how much of the body's surface is affected.
- Early signs often mimic the flu (fever, malaise) before the rash appears.
- Immediate discontinuation of the suspected medication is the most critical step for survival.
- Survivors must avoid not only the trigger drug but also chemically similar medicines to prevent recurrence.
- Long-term care often requires a team of specialists, including ophthalmologists and dermatologists.
Understanding the SJS and TEN Spectrum
Doctors view SJS and TEN not as two different diseases, but as a spectrum of the same severe reaction. The primary way they distinguish between them is by measuring the total body surface area (TBSA) where the skin has detached.
Stevens-Johnson Syndrome typically affects less than 10% of the body. It is often the "starting point" of the reaction. If the detachment covers between 10% and 30%, it is called Overlap Syndrome. When the damage exceeds 30% of the body, it is classified as Toxic Epidermal Necrolysis, which carries a much higher mortality rate-sometimes exceeding 30%.
These conditions fall under the broader category of Severe Cutaneous Adverse Reactions (SCAR). Essentially, your immune system overreacts to a medication and begins attacking the keratinocytes (skin cells), leading to full-thickness epidermal necrosis. This means the top layer of skin dies and separates from the deeper layers, leaving the body vulnerable to infection and fluid loss.
| Feature | Stevens-Johnson Syndrome (SJS) | Toxic Epidermal Necrolysis (TEN) |
|---|---|---|
| Skin Detachment (TBSA) | Less than 10% | More than 30% |
| Typical Mortality Rate | Approximately 5% | Often exceeds 30% |
| Primary Risk | Mucosal erosions and local infection | Sepsis and multi-organ failure |
| Hospital Setting | General ward or dermatology unit | Burn unit or ICU |
High-Risk Medications and Triggers
Not all drugs cause these reactions, but certain classes are notorious for them. Most reactions occur within the first eight weeks of starting a new medication, though some can appear weeks after the drug was stopped. It is important to note that the risk isn't just about the drug itself, but how it is administered.
For instance, Lamotrigine (an epilepsy and mood stabilizer) is a well-known trigger. The risk of SJS increases significantly if the dose is raised too quickly or if the medication is stopped for a few days and then restarted at the full dose without a gradual re-escalation. Similarly, Allopurinol (used for gout) and Carbamazepine (for seizures) are frequently linked to these emergencies.
Other common culprits include:
- Antibiotics: Specifically sulfonamides like Sulfamethoxazole.
- Pain Relief: Oxicam-class NSAIDs, such as meloxicam and piroxicam.
- Anticonvulsants: Phenobarbital and phenytoin.
- HIV Medications: Specifically nevirapine.
One dangerous trap for survivors is cross-reactivity. If you reacted to one anticonvulsant, your body might react similarly to another one because they share a similar chemical structure. This means a survivor of SJS caused by carbamazepine must be extremely cautious with other medications in that family.
Who is Most at Risk?
While anyone can develop these reactions, certain factors tilt the scales. Genetic predisposition plays a massive role; if a close family member has had SJS, your risk is higher. Immune system health is another factor. People living with HIV/AIDS or those undergoing chemotherapy are more susceptible because their natural defenses are compromised.
Interestingly, specific drug combinations can increase risk. For example, taking Sodium Valproate at the same time as lamotrigine can make a skin reaction more likely. Additionally, people who have a known allergy to trimethoprim may be more prone to these severe reactions when exposed to similar compounds.
Recognizing the Warning Signs
The window for intervention is small. The process usually unfolds in three distinct stages. First, you'll feel like you have the flu: high fever, muscle aches, and a general sense of malaise. This is the "prodrome" phase, and it is often ignored as a simple virus.
Within one to three days, the second stage begins. A red or purple rash appears, often starting on the torso and spreading outward. This rash is not like a typical itch; it is often painful to the touch. Soon, the rash evolves into blisters. These aren't just on the skin-they frequently appear on mucosal membranes. If you notice sores in your mouth, on your lips, or in your genital area along with a spreading rash, this is a critical red flag.
The final stage is the "sloughing" phase. The skin dies (necrosis) and peels off in large sheets, leaving the raw dermis exposed. At this point, the body loses its ability to regulate temperature and keep out bacteria, which is why the risk of sepsis becomes so high.

Survival and Long-Term Recovery
Treatment for SJS and TEN is primarily supportive. There is no single "cure" pill; instead, the focus is on keeping the patient stable. This usually happens in a specialized burn unit where sterile environments prevent infection. The most urgent step is the immediate removal of the drug that caused the reaction.
However, the battle doesn't end when the skin heals. The long-term complications can be life-altering. The eyes are particularly vulnerable. Between 30% and 50% of survivors experience ocular sequelae, ranging from severe dry eye and photophobia to corneal scarring and total blindness. Because of this, lifelong monitoring by an ophthalmologist is often required.
Other survivors deal with:
- Skin issues: Permanent depigmentation (white patches) or deep scarring.
- Respiratory problems: In severe cases, the lining of the lungs or esophagus can be affected, leading to esophageal strictures.
- Genital complications: Women may experience vulvovaginal stenosis, and men may develop phimosis.
- Hair and Nails: Diffuse thinning of scalp hair and nail dystrophy, though nails often recover over several months.
How do I know if a rash is SJS or just a normal allergy?
A normal drug allergy usually causes itchy hives or a mild rash. SJS is different because it is typically accompanied by a high fever and "mucosal involvement"-meaning sores in the mouth, eyes, or genitals. Most importantly, SJS skin is painful and eventually peels off in sheets, whereas a typical allergy does not cause the skin to die and slough off.
Can SJS happen if I've taken a drug for years?
While most cases happen within the first 8 weeks of starting a drug, it is possible for a reaction to occur later. Changes in dosage-such as a sudden increase in the amount of medication-can trigger a reaction even in someone who has been on the drug for a while.
What should I do if I suspect I have SJS?
Go to the Emergency Room (A&E) immediately. Do not wait for a GP appointment. Tell the medical staff exactly which medications you are taking and when you started them. The fastest way to stop the progression is to identify and remove the trigger drug.
Is there a way to prevent SJS?
While unpredictable, you can lower risk by following strict dose-titration schedules provided by your doctor, especially for drugs like lamotrigine. Avoid starting other new medications or changing your diet during the first three months of high-risk treatment to ensure any rash that appears can be easily linked to the primary medication.
Can you get SJS more than once?
Yes. Re-exposure to the original drug or a structurally similar drug can trigger a recurrence. This is why survivors must keep a detailed record of the causative agent and share it with every healthcare provider they visit.
Next Steps for Patients and Caregivers
If you are prescribed a medication known to carry an SJS risk, do not panic-the absolute risk for most individuals remains very low. However, be proactive. Ask your pharmacist for a clear list of "red flag" symptoms. Keep a medication log that includes the exact date you started a drug and any dose changes.
For those who have survived SJS or TEN, the priority is a multidisciplinary follow-up. Ensure you have a scheduled appointment with a dermatologist for skin grafts or scarring management and an ophthalmologist for corneal health. If you notice new dryness or blurred vision, seek help immediately, as ocular complications can progress rapidly even after the skin has healed.
Caroline Duvoe
April 22, 2026 AT 16:34basically just a summary of a medical textbook 🙄
Mayur Pankhi Saikia
April 23, 2026 AT 05:54Actually,, the TBSA percentages are far too simplistic for a real clinical diagnosis... any first year medical student knows the nuances of the overlap syndrome are way more complex than this basic guide suggests,,, honestly a bit amateurish!!
Rick Brewster
April 23, 2026 AT 19:51one must wonder if the very act of categorizing human suffering into percentages like ten or thirty percent doesnt strip the visceral horror of the experience from the clinical reality because in the end we are just organic matter reacting to chemical catalysts in a cosmic dance of biological failure where the skin is merely the veil that separates our inner fragility from a cold uncaring world and yet we treat it as a spreadsheet problem
Dave Edwards
April 23, 2026 AT 21:40Typical corporate health advice telling us to just 'go to the ER' as if the healthcare system actually works for the average person! 🙄 I bet the pharmaceutical companies are laughing while they push these high-risk drugs on us without any real warnings until after the damage is done! 😱
Mel Glick
April 24, 2026 AT 11:19The mention of cross-reactivity is absolutely crucial! People seriously underestimate how a similar chemical structure can trigger the same nightmare. You have to be aggressive about sharing your medical history with every single doctor you see or you're basically playing Russian roulette with your skin!
Sarah Watters
April 24, 2026 AT 14:19It's funny how these 'high-risk' lists always seem to omit the experimental stuff they're testing in certain regions. Pretty sure the triggers aren't just random genetic luck but specific batches designed for certain demographics to see how the immune system holds up under stress.
Mike Arrant
April 25, 2026 AT 10:18You guys are all panicking. Most people handle these meds just fine. If you're the type to Google symptoms and find a rare skin disease, you're probably already an overthinker who needs to stop obsessing over things you can't control. Just take your meds and stop acting like every rash is a death sentence.
Saptatshi Biswas
April 25, 2026 AT 23:14The absolute audacity of some people to dismiss this as 'overthinking' when the medical infrastructure in India is far more attuned to these severe reactions due to our diverse genetic pool! It is an absolute disgrace that Western perspectives often minimize the systemic trauma of TEN, which is a catastrophic failure of the body's primary barrier, leading to a level of agony that is simply beyond the comprehension of someone who has never seen a ward of burn victims!
Anantha Lakshmi
April 27, 2026 AT 16:09Let's stay positive everyone! 🌟 The most important thing is that we have the knowledge to catch it early. Awareness is the first step to survival and we can all support each other by staying vigilant and keeping those medication logs! 💪✨
Odicha ude Somtochukwu
April 28, 2026 AT 22:23I truly believe that sharing this information is a noble pursuit,, as it empowers the patient to be an advocate for their own health... Many in my community have faced similar struggles with medication access and side effects,,, and such a guide provides a necessary layer of safety for all!!
Ally Warren
April 29, 2026 AT 10:42The transition from the prodrome phase to the sloughing phase is a metaphor for the fragility of our existence. We believe we are solid and permanent, but a few molecules of the wrong drug can literally strip away our identity and our protection in a matter of days. It makes you realize that health is not a state of being, but a precarious balance that can be tipped by a single pill.